
Nitric Oxide for Solid Tumors
Nitric oxide is a short-lived, endogenously produced gas that has multiple mechanisms of action, depending on the concentration used. At a low concentration (<80 ppm), nitric oxide is a pulmonary vasodilator8; at a high concentration (<250 ppm), nitric oxide has antimicrobial properties9-12; and at an ultra-high concentration (>10,000 ppm), nitric oxide has been reported to show anticancer properties by activating innate and adaptive responses of the immune system.13

At Beyond Cancer, we have developed a proprietary system for the delivery of gaseous nitric oxide at ultra-high concentrations directly into solid tumors. Based on our current preclinical findings, we are developing treatment protocols using ultra-high nitric oxide concentrations to not only partially ablate primary tumors locally but also recognize and attack distant metastases systemically via stimulation of an antitumor immune response.

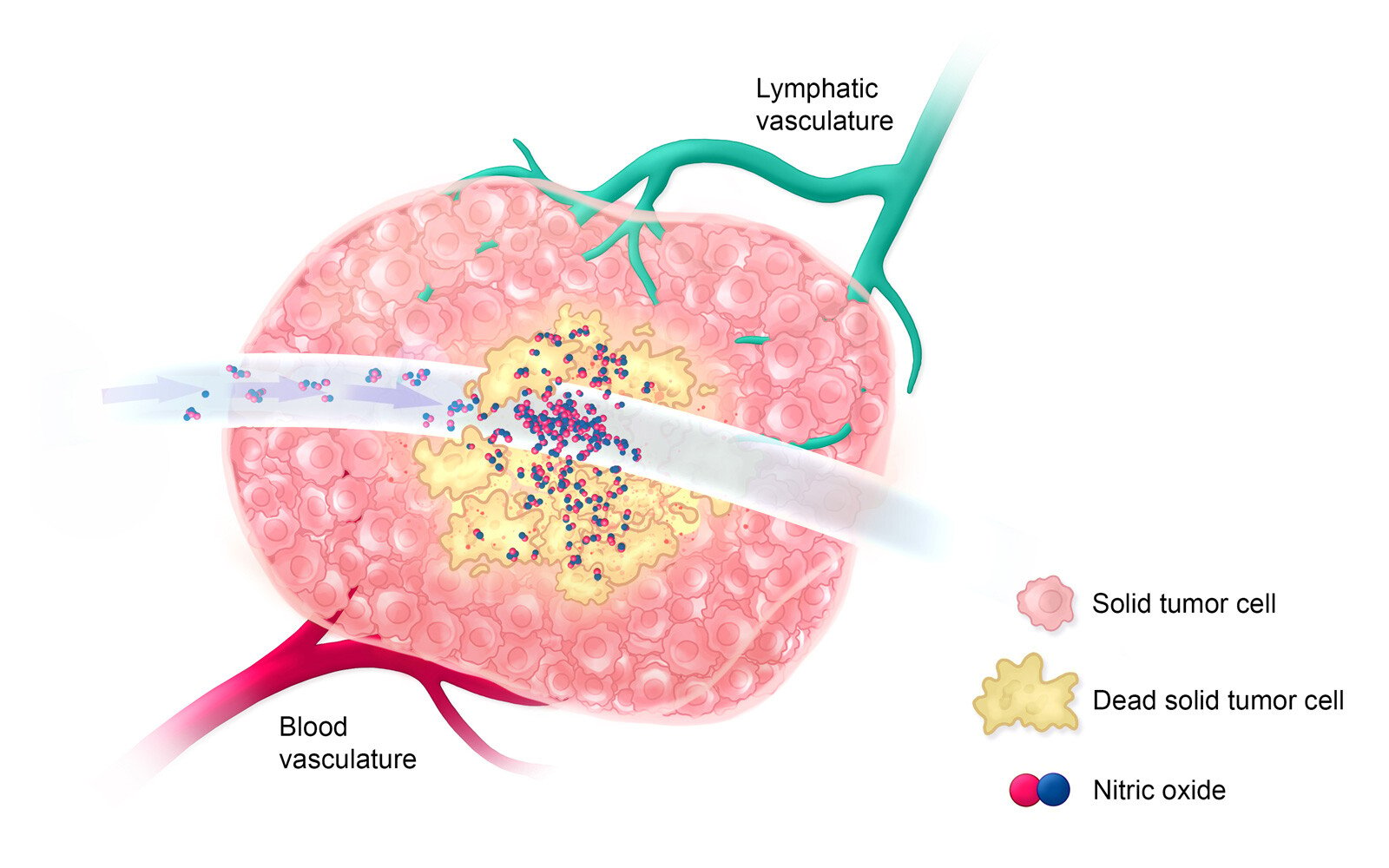
Treatment: Day 0
On treatment day 0, ultra-high-concentration nitric oxide is delivered directly into a large solid tumor for a short period of time to allow for the killing of all cells that it comes into contact with, only partially ablating the tumor.
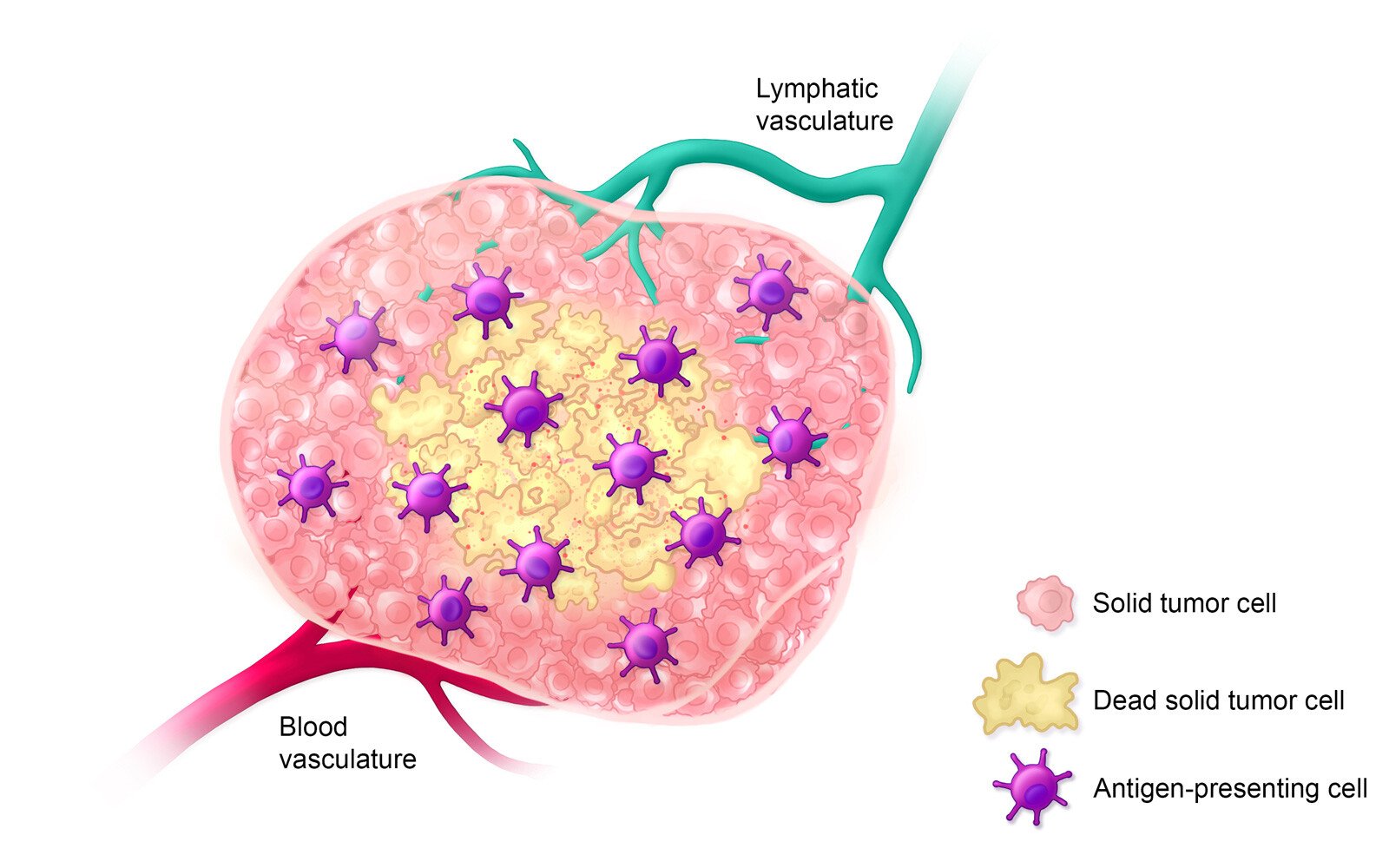
Estimated Timeline: Day 0-5
Within 5 days after treatment with ultra-high-concentration nitric oxide, antigen-presenting immune cells invade the tumor environment to detect and engulf dead solid tumor cells.
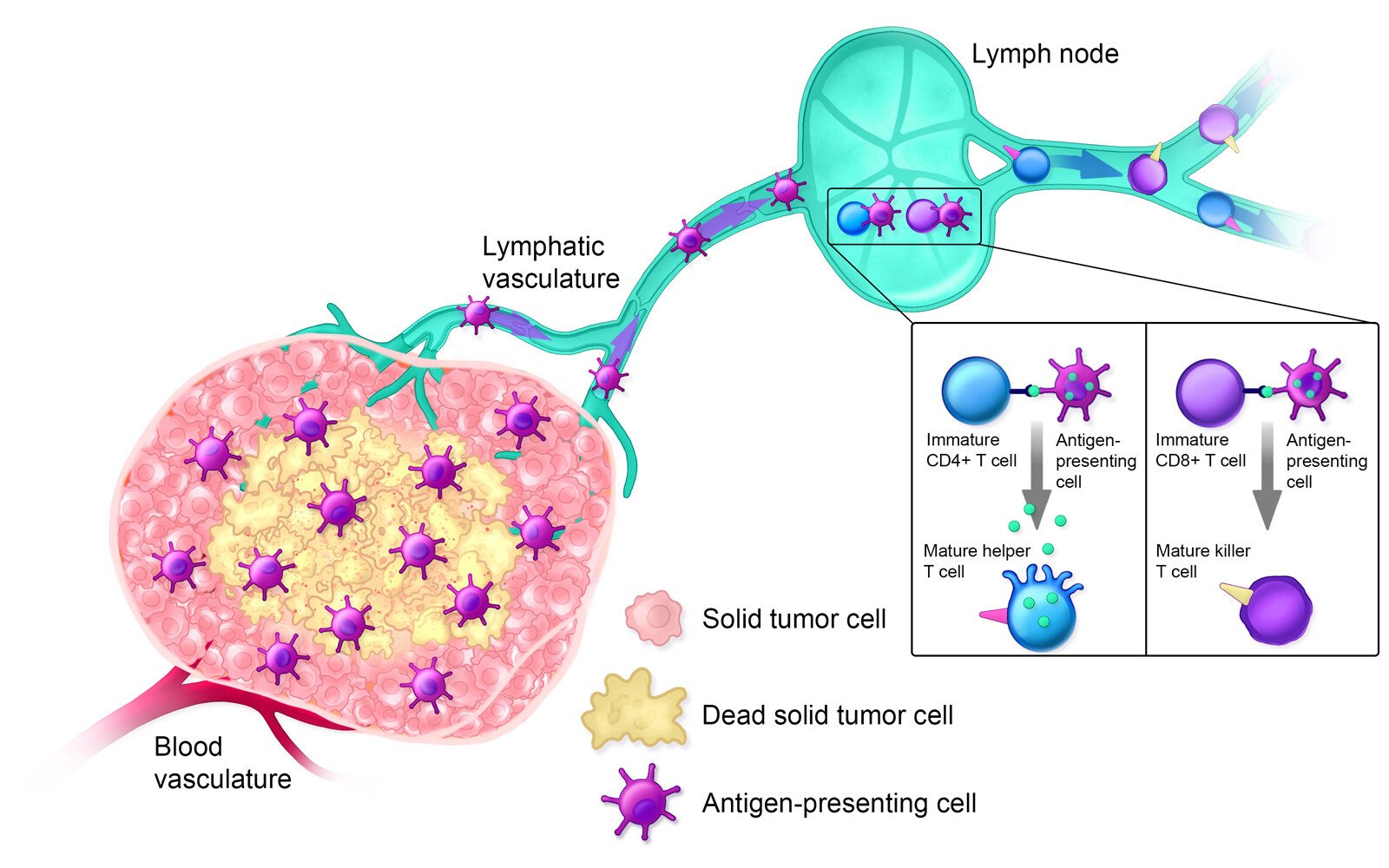
Estimated Timeline: Day 5-14
On days 5-14 after treatment, antigen-presenting cells inform the adaptive immune response by presenting antigens to immature T cells, thereby activating them.

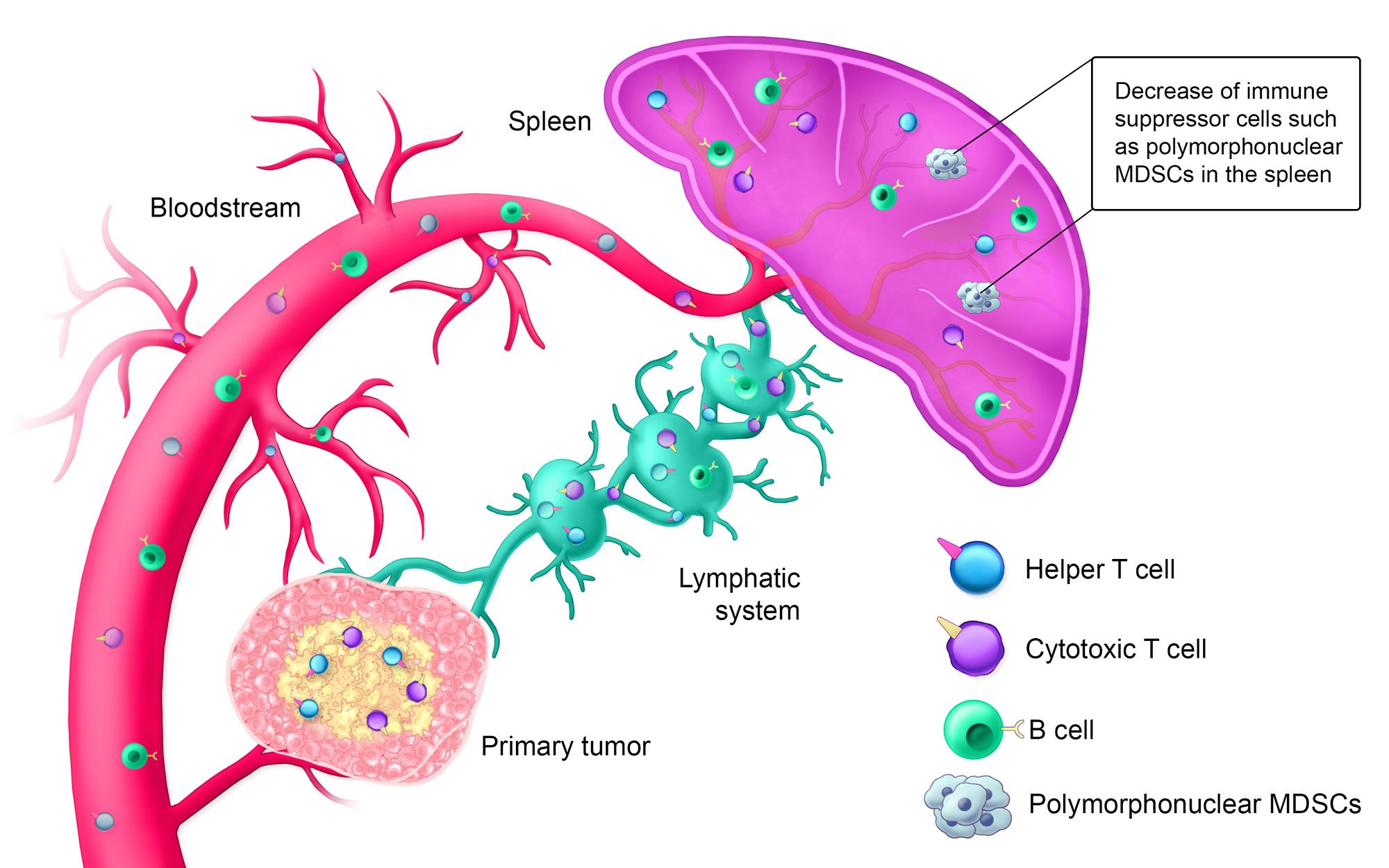
Estimated Timeline: Day 14+
Approximately 14+ days after treatment, the innate immune system is activated; helper T cells, cytotoxic T cells, and B cells are circulating in the bloodstream; and the lymphatic system is armed against the specific solid tumor type. Additionally, polymorphonuclear myeloid-derived suppressor cells (MDSCs), which suppress the immune system when tumors are present, are decreased in the spleen.



Significant reduction in the viability of mouse colon cancer cells after exposure to 50,000 ppm NO vs. air for 10-180 seconds.
Abbreviations: NO, nitric oxide; ppm, parts per million.
Significant time-dependent reductions in viability of mouse breast cancer cells after exposure to 150-50,000 ppm NO or air for 10-180 seconds.





Percentage of mice who were alive at day 45:
- 25% of naive mice
- 73% of mice who had received 20,000 ppm gaseous nitric oxide
- 100% of mice who had received 50,000 ppm gaseous nitric oxide

Abbreviations: NO, nitric oxide; ppm, parts per million.
Combination Therapy
UNO + anti-mPD-1
Key results
Day 9: Tumor volumes for UNO (5 or 10 minutes) + anti-mPD-1 treated mice were smaller than either anti-mPD-1 alone or UNO alone treated mice. (p-value = 0.0005 for 10 min UNO + anti-mPD-1 combination vs anti-mPD-1 alone.)
Day 100: 53% of mice treated with 50,000 ppm UNO for 10 minutes plus anti-mPD-1 were primary and secondary tumor-free. Survival was increased when treated with 10 min UNO and anti-mPD-1. (p-value = 0.0653 for 10 min UNO + anti-mPD-1 combination vs anti-mPD-1 alone.)
Study design: CT26 tumor-bearing mice were induced with a secondary tumor two days before UNO treatment and treated with anti-mPD-1 two days before UNO treatment. Mice received 4-5 anti-mPD-1 treatments. Tumor volume and survival were monitored.


TUMOR VOLUME AT STUDY DAY 9 - DIFFERENCE BETWEEN TREATMENT GROUPSa
| Treatment Group | n | Adjusted Mean (SEM) | Adjusted Mean | 95% CI | p-value |
|---|---|---|---|---|---|
| Anti-mPD-1 | 16 | 446.28 (68.73) |
NA | NA | NA |
| NO 50,000 ppm 10 min + Anti-mPD-1 |
15 | 100.43 (68.74) |
-345.85 | (-538.09, -153.62) | 0.0005 |
aAnalysis via mixed model repeated measures (MMRM) with fixed effects for baseline tumor volume, study day, treatment by study day interaction.
Some timepoints combining data from different measurement days (day 2 = 1+2; day 5 = 4+5; day 7 = 6+7; day 9 = 8+9)

